Careers, Sponsored Editorial, Your Career
Watching the Future of Clinical Research Unfold: From a Writer’s Desk
Editorial Staff

I still remember the stack of dense, jargon-filled trial protocols that landed on my desk a few years ago. As an in-house editor writing about biopharma and clinical trials, I was tasked with translating complex science into something patients or general readers could grasp. Back then, “patient-centricity” was a buzzword, and we often struggled to simplify consent forms or lay summaries. Today I look up from my computer and feel like I’m seeing a different world.
Modern trials increasingly use virtual visits and smartphone apps, and ethics review boards now expect clearer communication up front. From my writing chair, I’ve watched this transformation step by step, and I still marvel at the changes we’ve lived through.
Embracing Hybrid and Digital Trials
Before the pandemic, fully decentralized trials were rare. The FDA had noted that only a handful of studies operated entirely remotely in 2017-18. But then COVID-19 hit. In 2020, trial sponsors scrambled: lockdowns and social distancing suddenly made on-site visits impossible. We saw regulators and researchers pivot almost overnight.
Emergency FDA guidance explicitly urged the use of remote methods wherever possible. The result: hybrid trials exploded. One industry report notes that hybrid designs leapt from 20% of studies in 2019 to nearly 60% by 2021, with even more in the pipeline. In practice, this means parts of a trial (like enrollment or follow‑up questionnaires) now happen online or at home, with occasional clinic visits when needed.
My own work is flooded with stories about app-based monitoring and e-consent. It makes sense: surveys show that roughly 88% of adults (ages 23-83) are comfortable using mobile apps, and almost half have already used technology to communicate with their doctors. Patients typically carry smartphones or tablets, so why not use them for trials? Digital health tools promise big benefits: faster recruitment, better retention, and lower costs.
As one industry source puts it, technologies that let participants “contribute from home” can vastly improve engagement and even study diversity. In other words, we’re no longer limited to recruiting people who can drive to a hospital; we can reach people nationwide via the internet, making trials more inclusive and efficient.
It’s also become common for trials to use interactive electronic consent. I’ve seen consent videos and online modules replace some of the paper drudgery. A recent analysis reports that adding infographics, videos, and even chat‑group support to consent forms dramatically boosts patient understanding and satisfaction. For example, one study noted that volunteers retained more information when they used a multimedia consent tool (with step-by-step visuals and FAQs) than when they just listened to a lengthy phone call. The pandemic showed us that tools like tablets, telemedicine, and home shipping of drugs aren’t gimmicks; they were essential to keep trials going. Now they’re proving their worth by lowering travel burdens on patients and reducing missing data.
Putting Patients First in Research
The language around trials has also shifted. In the past, the “study coordinator” might make unilateral decisions and merely inform patients of the rules. Now teams routinely consult patient communities and advocacy groups during trial design. Partnering with patient organizations to foster a sense of shared responsibility and co-creation in research.
Language, in particular, matters enormously. Using clear, concise, and easily understandable wording empowers participants and fosters transparency, trust, and mutual respect between researchers and patients. Indeed, we’ve found that swapping scientific jargon for plain language can dramatically improve comprehension. Instead of a handout filled with Latin terms, many studies now give participants well‐illustrated flyers or short videos.
Translation and interpretation services are routine, too: trial information must often be available in multiple languages to ensure equitable access. These changes aren’t just niceties. Research shows that when participants are better informed in their own language, recruitment improves and so does participants’ trust in the process. In short, designing trials around patients’ realities is no longer optional; it’s central to ethical research.
Plain Language and Transparency
Closely tied to patient-centric design is the drive for transparency. Today, there’s growing momentum around publishing trial results back to participants in ways they can actually use. A landmark move came with the European Clinical Trials Regulation, which now mandates a lay-language summary of trial outcomes. These summaries must be written at about a 6th-8th-grade reading level and avoid jargon, so patients and the public can understand what was found. It’s a sea change: previously, many volunteers never even heard about the results of studies they joined. In fact, a global survey found that while 72% of participants wanted to know trial outcomes, nearly two-thirds had never received any summary. That gap is closing. Pharmaceutical companies, journals, and regulators are increasingly requiring plain-language summaries alongside any published results.
As an editor, I’ve noticed how this emphasis on clarity resonates with readers. Whenever I wrote a brochure or a press release, I’ve learned to put myself in the audience’s shoes, and that often means reordering the material to highlight what matters most to a patient (outcomes, side effects, and next steps) before the technical details.
It also means being transparent about uncertainties. For example, trial websites now often include Q&As or short videos explaining why a placebo might be used, or what eligibility criteria mean in practice. This kind of openness builds trust. Even outside formal trials, new tools echo these values: for example, platforms like ClickClinicals℠ (which helps nurse practitioner students start their search for clinical preceptors) that “clear communication” and “transparent communication” are at the heart of its service. Whether it’s matching students to mentors or recruiting patients to studies, the message is the same: no one likes surprises. Giving people straightforward information early and often is now seen as essential.
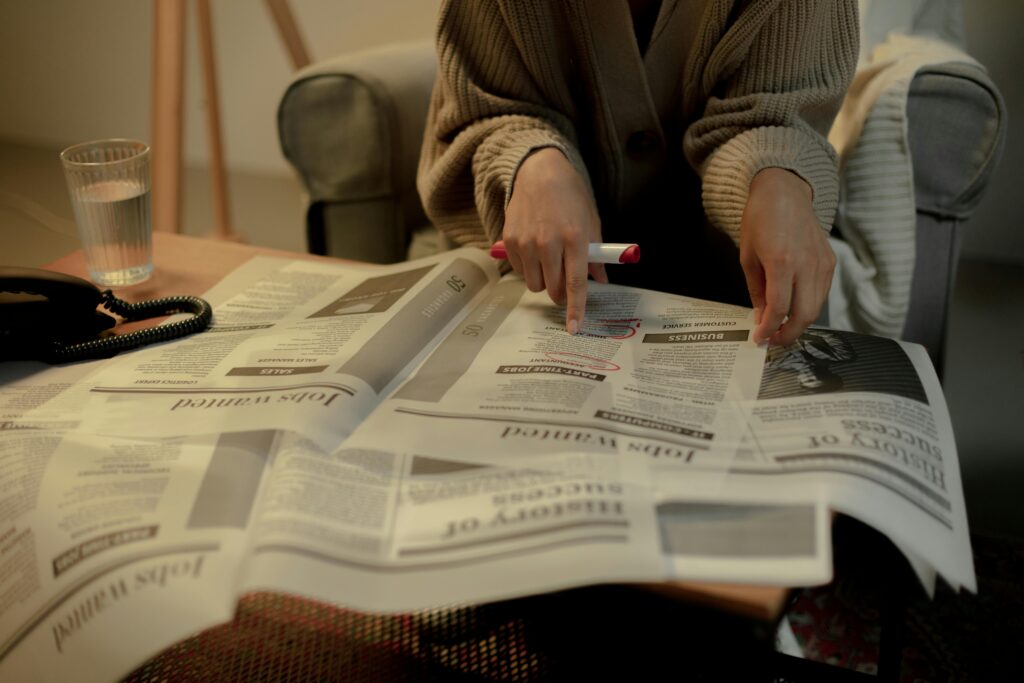
The role of good communication is obvious in person, too. A clinician might hand a participant an easy‐to-read consent form or show a chart on a tablet. I often think of a photo I saw recently: a friendly research nurse explaining paperwork to a trial volunteer, one-on-one. This human contact, combined with plain language materials, really embodies the change we’ve been part of. It’s the opposite of the old model, where patients got a sheaf of dense pages; now the packet is short, the nurse is patient, and the participant is actually asking questions.
Technology and the Human Touch
From my desk, I’ve seen labs adopt AI to sift trial data, wearable devices to track patients, and even video games to improve motor skills in therapy trials. And yet what remains constant is the human drive behind it. Writing for a general audience, I’ve had to learn about these tools, but I never lose sight of the people they serve. In the next decade, I expect we’ll see even more personalized trials (think AI-tailored medicine and virtual reality consent tools) and, with them, more emphasis on compassion and clarity. The future of clinical research is undeniably high-tech. But the best stories I get to tell are always about how that tech helps real people: making trials more accessible, more transparent, and more humane.
SEE ALSO: Can Kratom Help You Study? What Students Should Know Before Trying It